The government loves forms.
Forms denote rules and rules require bodies in seats to read the forms and enforce the rules. Sometimes, forms are standardized; other times, you’re free to create your own. While this may seem odd remember that in certain cases the rules exist simply as required content. The manner in which content is arrayed on a page is less important.
But what happens if you don’t know the rules, or if the rules are complicated? What do you do when there are multiple forms from which to choose and yet no official guidance on which one is best? Even worse, what happens if you depend on other people to help you fulfill the rules, and those people don’t know what they’re doing?
It is within this context that we focus on the Medical Necessity Certification Statement, or MNCS. The form has had many names over the years, including Physician Medical Necessity Certificate (PMNC), Certificate of Medical Necessity (CMN), and even now can be either a Physician Certification Statement (PCS) or Non-PCS, if signed by an approved individual who is not the physician.
The rules surrounding the many variations of this form are often misunderstood and can create billing challenges if not properly followed. Yet, in our experience, the bad reputation that sometimes follows the MNCS is undeserved.
In this article, we will review when a MNCS is needed, who can complete it, how it is properly executed, and the most common reasons people get it wrong.
Origin of the MNCS
The origin of the MNCS can be found in the Code of Federal Regulations, specifically, 42 CFR §410.40(d). Here, the ground rules are laid out for two very different classifications of non-emergency transports, repetitive and non-repetitive.
We’ll define these momentarily, but for now, it’s interesting to note that what the regulation refers to is a “written order,” not a particular standardized form. And this written order is intended to substantiate the medical necessity of the ambulance transport.
Given this is the actual purpose of a MNCS we should review some key foundational elements, which are likely familiar to you by now.
Medical Necessity
Located in the same section of code, we find the following:
“Medicare covers ambulance services if they are furnished to a beneficiary whose medical condition is such that other means of transportation are contraindicated. The beneficiary’s condition must require both the ambulance transport itself and the level of service provided, in order for the billed service to be considered medically necessary.”
“Non-emergency transportation by ambulance is appropriate if either: the beneficiary is bed confined, and it is documented that the beneficiary’s condition is such that other methods of transportation are contraindicated; or, if his or her medical condition, regardless of bed confinement, is such that transportation by ambulance is medically required.”
“Thus, bed confinement is not the sole criterion in determining medical necessity of ambulance transportation. It is one factor…”
Bed Confinement
Remember, for a beneficiary to be considered confined to a bed, all three of the following criteria must be met:
- Unable to get up from bed without assistance, and
- Unable to ambulate, and
- Unable to sit in a chair or wheelchair
Provided the patient is bed confined before and after transport, with a valid reason explicitly documented and supported by all associated paperwork, bed conferment may be permitted to be used in and of itself to demonstrate medical necessity (though nothing is guaranteed).
We emphasize “may” because we have found that, even if a patient is bed confined, if he/she does not require an attendant (meaning the patient is conscious, alert and oriented), Medicare may deny.
When is a MNCS Required?
The need to obtain a MNCS applies to:
- Beneficiaries covered by Medicare, as well as other insurances that enforce this stipulation
- Non-emergency transports. Can be scheduled or unscheduled. Classified into two categories: repetitive and non-repetitive.
- Patients under the direct care of a physician.
Of note, for patients who reside at their personal residence or in a facility, and who are not under the direct care of a physician, a MNCS is not required. Of course, these are infrequently encountered scenarios, and providers may find it somewhat unnecessary to try to remember these exceptions. But it’s good to know the rules.
Format
There is no standard format, just mandated content. Ambulance services are free to create their own form, and many do.
As one Medicare Administrative Contractor, or MAC, states on its website, “it can be simply a written statement that supports the need for ambulance services.” Yet, anyone with experience will attest to the fact that something more than the vague “written statement” is needed. Winging it probably won’t suffice.
This is why that same MAC goes on to recommend the following:
- Include a space for narrative description from the physician
- Include pertinent medical information to help substantiate medical necessity
- Include fields for signatures and dates by authorized personnel
- Ensure continuity between the information in the MNCS with that found in other elements of the claim record, such as the PCR and diagnosis code
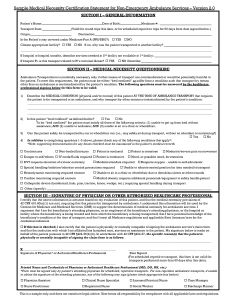
All of this stated, it is one thing to make content recommendations, but it’s another to assemble that content into a coherent and repeatable format that all stakeholders – the physician or other approved signer, ambulance service, billing office, and Medicare reviewer – can easily understand.
this reason, we recommend the MNCS template created by the experts at Page, Wolfberg & Wirth (PWW). A sample, courtesy of PWW, is available for download on their website – pwwemslaw.com.
Does a properly executed MNCS equate to payment?
No. As a standalone document, a properly executed MNCS does not mean the transport will be viewed as medically necessary, or get paid. Such determinations are based upon all program criteria being met.
This depends on the totality of the documentation, including relevant information captured during call intake, recorded in the PCR, indicated in the MNCS, and contained throughout the patient’s medical record.
Repetitive Transports
A little earlier, we mentioned two classifications of non-emergency transports. This distinction is important, because the rules for each are unique.
Transports are considered repetitive if a beneficiary requires three or more of them during a 10-day period, or at least once a week for at least three weeks. The rules for these types of situations are strict:
- MNCS must be signed and dated by attending physician
- MNCS must be signed and dated prior to service
- MNCS is valid for sixty (60) days from the date signed
Non-Repetitive Transports
It reasons that all other scenarios fall into this classification. These rules enable a bit more flexibility, but are still clear:
- MNCS may be signed by attending physician or an appropriate alternate person
- MNCS should be obtained at time of service, but there is a 48-hour window after transport
- MNCS is valid for sixty (60) days from the date signed
In those cases when a MNCS cannot be obtained by the physician either at the time or within 48 hours after transport, an authorized alternate signer can execute the form.
Such an individual must be an employee of the attending physician, hospital or facility where patient is being treated and from where the patient is being transported. He or she must also have personal knowledge of the patient’s condition at the time the transport is ordered or furnished.
Approved alternate signers include the following:
- Physician Assistant (PA)
- Nurse Practitioner (NP)
- Clinical Nurse Specialist (CNS)
- Registered Nurse (RN)
- Discharge Planner
Of note, if a discharge planner is going to sign, he or she is beholden to the same qualifying criteria. It’s worth noting that identifying who a discharge planner is can sometimes prove difficult.
In an institutional setting, the person fulfilling the role of a discharge planner may in fact bear the title. In other cases, a person who is designated by another title may also function in the capacity of a discharge planner.
In any such case, this person should legibly sign his or her name (and print it as a safety measure) and clearly indicate his or her applicable credentials and/or title.
We recommend ambulance services maintain accurate records of the titles and functions of the individuals signing non-repetitive MNCSs. This is especially so when it comes to someone signing in the capacity of a discharge planner. Such documentation can help demonstrate to a MAC that the person has a work history in said role.
When a MNCS Cannot be Obtained
Also, for non-repetitive scenarios, there may be a time when a MNCS simply cannot be obtained, such as when a physician or facility is unresponsive to multiple requests. In such cases, an ambulance service may bill without a MNCS, but only if the following conditions are met:
- If unable to obtain a MNCS within 21 calendar days from the date of service, and
- If attempts to obtain a MNCS are documented.
An acceptable form of documentation would include a signed return receipt or “proof of mailing” from the USPS or other similar service demonstrating delivery of the letter.
Common Mistakes
The truth is it’s easy to mess up a MNCS. So many factors need to come together and work in harmony in order for a MNCS to be properly executed. And basically all of these are outside the control of an ambulance service.
Yet, the ambulance service bears the burden of making sure the MNCS is properly executed. Considering this, we have to get it right. This means knowing how it can go wrong. So let’s examine the most common mistakes people make.
Dates
Our first most common mistake is the MNCS is not fully dated. Sometimes the requested date of transport is included, but the signature itself is not dated.
In certain repetitive cases, both fields contain dates, but the signature date is not indicated prior to the transport itself. That’s a non-starter.
In some cases, there are no dates at all!
Remember, there are two very different and equally important date fields: the date of requested transport, and the date of signature. Both must be completed.
Another mistake is when a signature is dated, but the first requested date of service is greater than 60 days away. A MNCS is good for 60 days, between the same locations and for the same reasons. In other words, one MNCS can be used for multiple transports within this span of time, but not exceeding that span of time.
Signatures
You may have guessed it, but much like a MNCS sometimes isn’t dated, one of the more common mistakes is a MNCS isn’t signed.
Yet there are many ways in which a signature can be included, and still be insufficient.
For instance, a MNCS may not be signed by the appropriate person. This again highlights the different requirements for repetitive and non-repetitive transports.
In other cases, a signature can be legible and from an appropriate person, but not indicated in the appropriate field.
And of course we have issues with legibility. Physicians can be notorious for their indecipherable signatures, which at times may resemble an EKG for atrial flutter more than an actual human name.
Give this example a read and see if you can guess the name.
We’ll reveal the answer a bit later.
Fortunately, illegible handwriting isn’t the death knell of a good MNCS. Consider the following practices, all of which are acceptable when dealing with illegible signatures:
- Initials over a printed name
- Illegible signature over printed/typed name
- Illegible signature accompanied by signature log or attestation statement
On this last point, many ambulance services struggle with physicians, nurses, and other healthcare professionals who routinely write illegibly. Some agencies utilize signature logs and attestation statements as tracking systems, in the event these signatures are called into question.
Ambulance services have varying opinions on committing to their use, in part because it can be challenging to ensure records are kept current as healthcare professionals from the facility in question come and go.
Despite this, if these types of transports constitute a significant portion of business, and legibility is an ongoing challenge, then doing a little more paperwork may be a wise investment of time and effort.
A sample signature log and attestation statement, again courtesy of the experts at PWW, is available for download at www.pwwemslaw.com.
Lastly, it’s important to clarify that electronic signatures are acceptable, but stamped signatures are not. An electronic signature is still one that is hand signed, but instead of applying ink to a sheet of paper, a person may use a stylus or a finger, capturing the movement on a computer screen.
Credentials
Not to border on redundancy, but again we find that a very common mistake is when something is left out entirely – this time, credentials. In other cases, we find credentials are indicated but are not legible. Also, credentials are often indicated and legible, but not in appropriate field.
Also, it’s worth pointing out “Dr.” is a title, not a credential. A credential is MD, DO, RN, etc.
Questionnaire
Generally, we find that something is written in the narrative field designed for freehand description of the patient’s condition, and why the patient needs transported by ambulance. However, that information is often rather thin and can leave room for doubt in the mind of a Medicare reviewer.
This space should contain precise and relevant detail, and should not contradict other parts of the Medical Necessity Questionnaire.
For instance, the first question following the narrative field is about bed confinement. And bed confinement, as we noted earlier, has three specific criteria, all of which must be met. So, if bed confinement is selected, the narrative description should depict a condition which supports this.
This applies for the next question as well, which asks if the patient can be transported by other means. If the patient is bed confined, it wouldn’t make sense to indicate yes; nonetheless, busy facility personnel may not realize this at the time.
The purpose of a MNCS is to support the medical necessity of the transport, but if the information it contains is self-contradictory, it will not fulfill its purpose.
Record Keeping
Outside of transports that fall under the prior authorization demonstration program, Medicare does not read a MNCS prior to processing a claim and then decide whether or not it is acceptable. For the most part, the system is automated, and once claims are coded, they are submitted and paid electronically.
The system is in many ways based on honor. Medicare trusts that an ambulance service has done its part, and is not knowingly submitting claims without a MNCS, or without proof of having made an attempt to obtain a MNCS for those non-repetitive transports when a MNCS could not be obtained within 48 hours.
The responsibility is on the ambulance service to obtain the paperwork prior to submitting the claim, and then to hold onto that paperwork, in the event it is requested at some later point, during a post-payment review.
That Signature
As for that mysterious signature, would you have guessed it belongs to Donald Trump? If so, there may be a spot open for you at Medicare reviewing MNCS forms.
Contact Us
Cornerstone Adminisystems is an employee-owned provider of billing, compliance and revenue cycle management services to the EMS and medical transport community. Contact us for help improving your revenue cycle.
For resources designed to maximize your EMS agency’s reimbursements, check out our free tools for downloadable guides and forms.